
Who's Running This Thing Anyway?

“Oh. My. God. Enough already. It’s VTach. Ok? Move on and treat the patient,” you hear as you walk into your shift.
As you enter the ER, you see the residents gathered around the teaching whiteboard with the chief resident holding up an EKG. You also see a very frustrated intern who is a little fed up, as evidenced by his outburst.
“And now, this intern is going to talk us through this EKG and why he is so convinced that this is Ventricular Tachycardia” you hear the chief resident say with a glare.
“There’s 25 in the waiting room, 5 in rooms to be seen and this ‘5 minute pearl’ has been going on for 15 minutes already” the intern exclaims. “I’m so-”
“What’s going on?” you ask, cutting in and trying to diffuse the situation. “Anyone want to catch me up on this case?”
“Sure! I will” one of the medical students tells you, oblivious to the tension in the room. “This was a patient we had today in room 9. 57-year-old male coming in with chest pain. He didn’t look great. A little pale and sweaty. Medics said that he was in normal sinus for them but then jumped into this rhythm right as they walked into the ER. They managed to capture an EKG as they walked down the hall to his room. Want to take a look?”
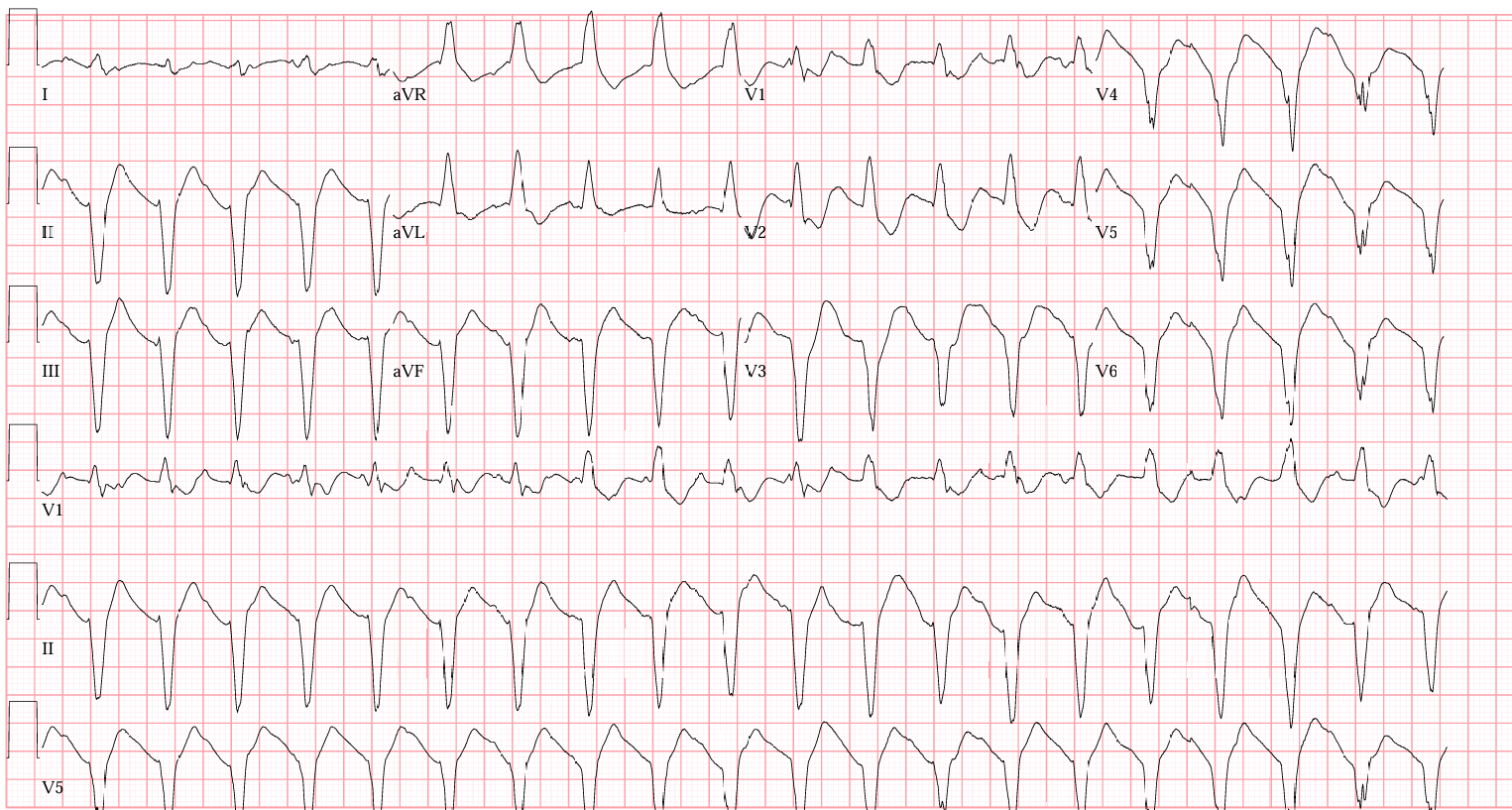
Rate: 135 ish
Rhythm: Not sinus, that’s for sure
Axis: Left axis
Intervals: Wide QRS, no PR interval
Morphology: Wide complex tachycardia. Sure looks concerning. There’s a finding in this EKG that’s diagnostic of VTach, but we’ll get to that in a minute. In fact, it’s probably the chief resident’s teaching point…
Final Read: This sure looks like VTach to me
“Wow, that looks bad!” you say to the medical student. “So, what happened next?”
“Well, Sir, the patient looked extremely unwell. We moved him over from the EMS stretcher to the hospital bed and he rapidly went unresponsive and pulseless. We emergently defibrillated him and he popped right back up! He was talking to us and everything. Actually, he was kind of yelling at us a bit because he thought we hit him. His repeat ECG showed a massive STEMI, we activated the cath lab and they took him right up. Really interesting patient.”
“Thank you, medical student, for that excellent summary,” the chief says, “But now, the intern is going to explain to the attending and everyone else in the room why we knew this was Ventricular Tachycardia and not something else. Aren’t you?”
“I mean, it’s pretty obvious, right? The guy had chest pain, he looked terrible, went into a wide complex rhythm and then went unresponsive. After one shock, massive STEMI, right to the cath lab. What else could it be?”
“So,” the chief starts, “In this case I agree with you. I would always assume this was VTach in this specific scenario but it isn’t always that obvious. There are some clues in the EKG that can point you in the right direction. Let’s start with this strip as a warm up. Tell the group what you’re seeing here. It’s from a pediatric patient who was 3 days old, so even though it looks narrow, I promise it’s wide:”
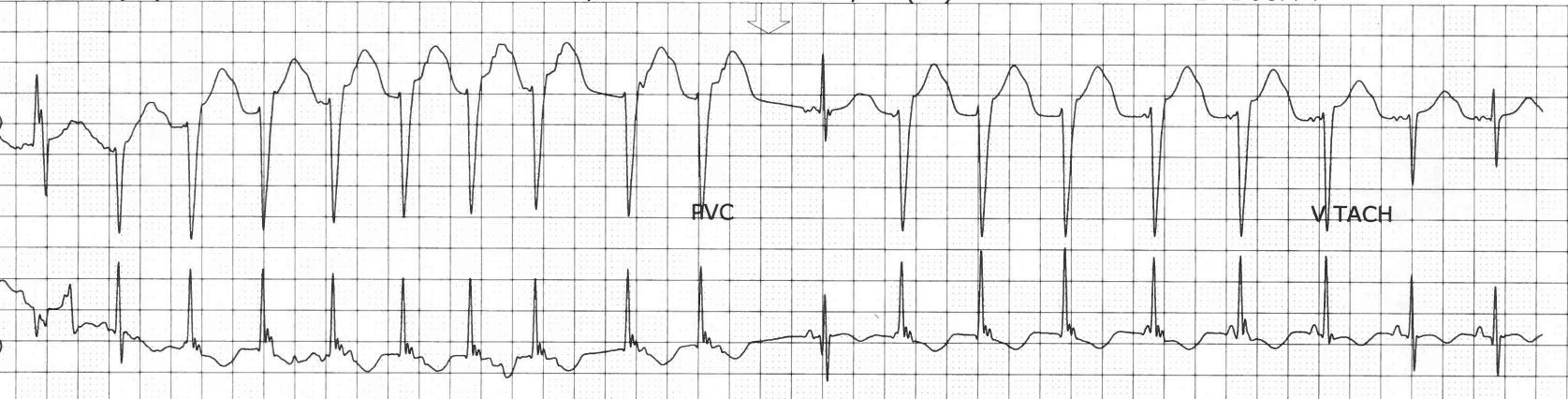
“Well. Uhhh.. It’s a wide complex tachycardia.” He starts.
“But is it Vtach? Or something else?” the chief asks with a smirk.
“It’s… Uhhh.. I think…” he stammers.
“Come on, dude! I thought this was easy and we were wasting your time!” she says. “Which is it? Vtach? Or something else?”
The chief lets the intern struggle for a bit and then takes over. “What you’re seeing on this strip is ventricular tachycardia. The first beat is a fusion beat and the eleventh beat is a capture beat. Remember, if you see fusion beats and capture beats in the middle of a strip of a wide complex tachycardia, think VTach every time. I’ve marked it up for you to review:”
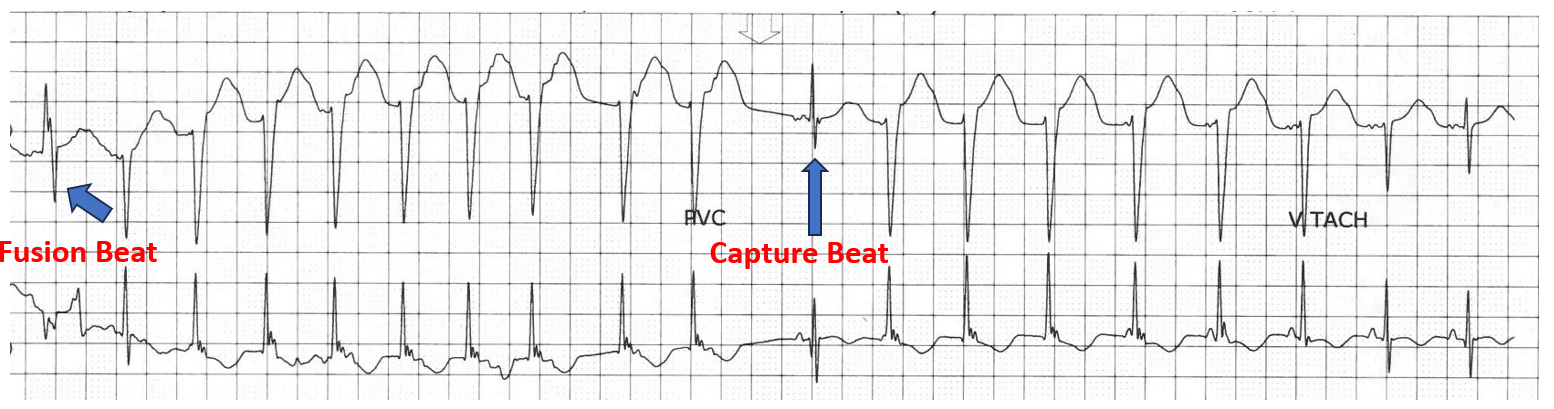
“Remember, a fusion beat occurs when the ventricles and the SA node fire at the same time causing a ‘fusion’ of the two beats and a capture beat occurs when the SA node temporarily recaptures electrical control of the heart,” she says. “Again, both of these beats tell you what you’re seeing is VTach. Now here’s another example from a recent tele strip. See the capture beats in the middle?”

“Now what about the first EKG? What am I seeing that is diagnostic for VTach there? It’s not just his story.” She asks the intern.
“You win; I’m not sure,” he tells her, starting sheepishly at his feet.
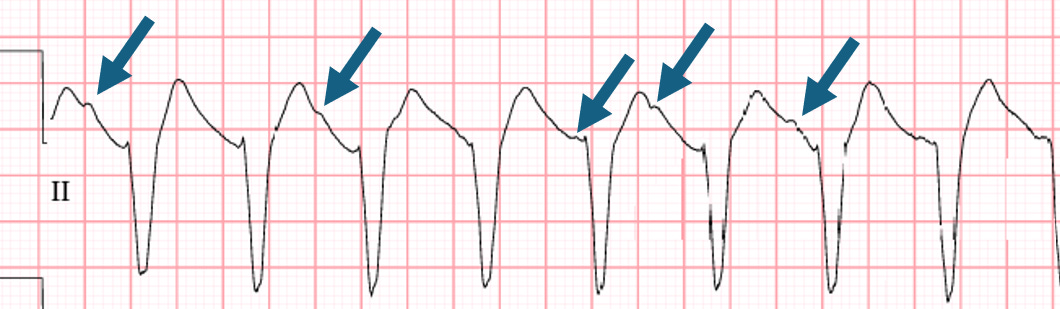
“Look closely at the morphology in the rhythm strip for lead II. Do you notice how there are some bumps that seem out of place? Those are p waves. This ECG shows you A-V Dissociation, which is diagnostic for VTach. Here, I’ve marked some of the p waves for you with blue arrows. Now let’s get back to work everyone.”
Case Wrap Up:
For more information and tips on how to tease out if a wide complex rhythm is Vtach or something else, see this interesting article in the Journal of Clinical Medicine from 2023!
Recap:
VTach is my favorite dysrhythmia
Capture beats and fusion beats should push you towards a diagnosis of VT
AV Dissociation is diagnostic for VT
Hit me up with any questions,
Lloyd
**Looking for a dynamic guest lecture on Emergency Cardiology for your Grand Rounds? Reach out here for a lecture request by Dr. Tannenbaum. If you have reached out already, I have emailed you back. If you haven’t gotten it, please message me directly on Substack or just reply to this email.**
_________________________
Lloyd Tannenbaum, MD