
She's Shaking; It Must be a Seizure!

“Hey, can I staff the patient in bed 12 with you? This one is a little strange.” You hear your intern ask the senior resident.
“Sure!” She says, “What’s going on with your patient?”
“Well. He’s a 95-year-old male coming in with a first-time seizure today.” The intern starts.
“WHAT? I’m going to stop you right there.” She asks skeptically. “A first-time seizure? Are you sure? At 95?”
“Right.. I told you it was a strange case…” the intern continues. “He was with his daughter at the time. She said he was sitting on the couch and then suddenly went unresponsive. She noticed some shaking of his limbs. It lasted maybe 1-2 minutes and then he woke right back up. The daughter says he has no idea what happened. He was confused for maybe a minute but then went right back to normal. She was a little concerned, but since he was acting normally, she decided to just call the family physician.”
“Ok… then what?” The senior asks.
“Well, this is when it gets a little strange. He had 3-4 more episodes of this at home so she called 9-1-1 when she didn’t hear back from the doctor’s office.”
“So. He’s in status? What’s his exam like?”
“Uhhh… Totally normal?” The intern says and looks a little worried.
“WHAT?” the senior says. “You’re telling me that you have a 95-year-old male who developed a new seizure diagnosis TODAY and had 4-5 seizures but a totally normal exam and is just sitting in his room feeling totally fine?”
“Yes Ma’am. I was hoping you could come with me and take a look? I ordered bloodwork and a head CT. I feel like I’m missing something…”
“Here’s his ECG!” the nurse comes in, interrupting the intern’s uncomfortable moment.
“Let me take a look at this ECG while you reflect on what you just told me and try to broaden your differential,” the senior tells the intern with a bit of a glare.
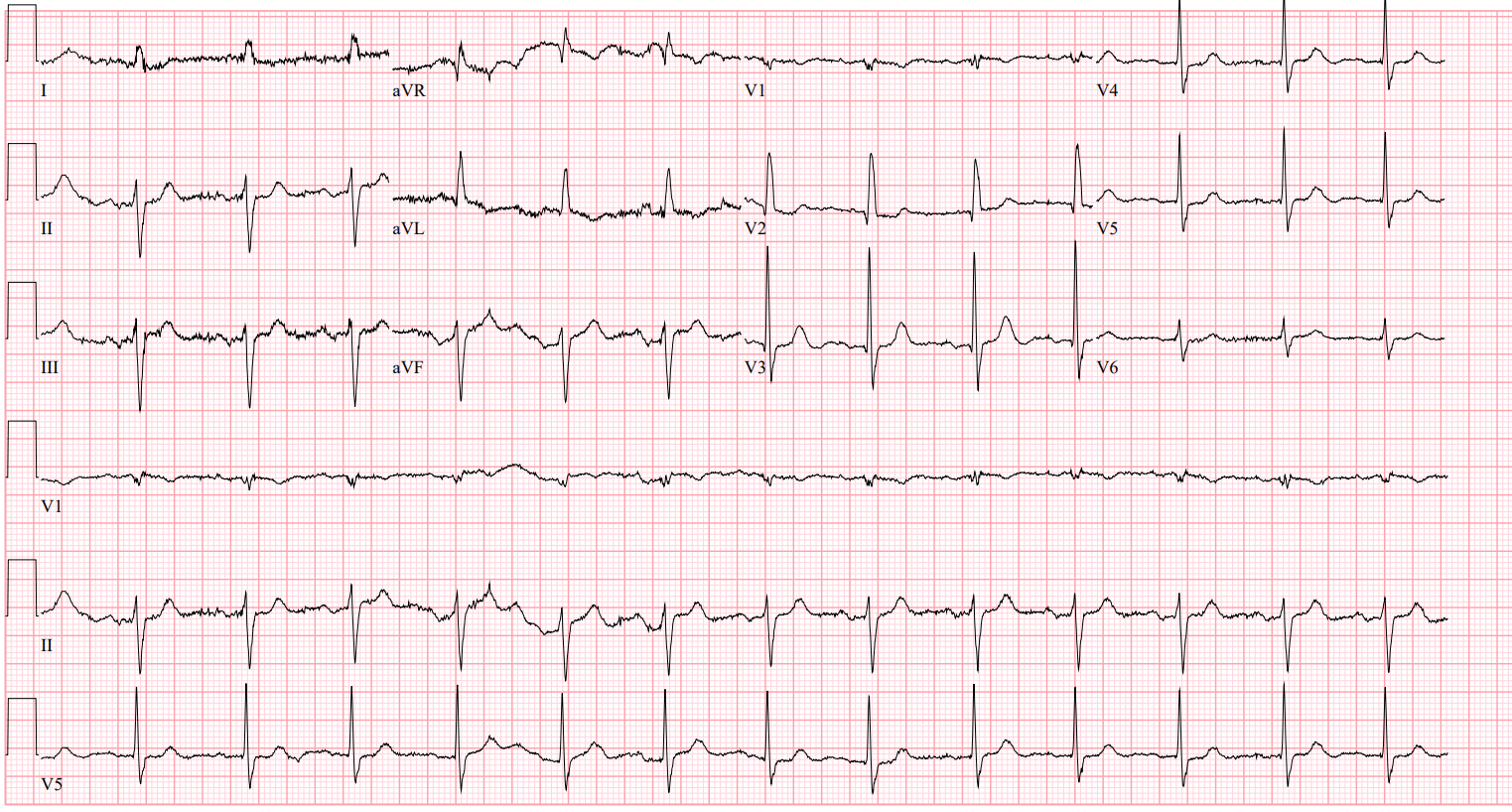
Rate: 80
Rhythm: Sinus rhythm
Axis: left axis
Intervals: narrow QRS complexes, QTc looks ok, PR is maybe a touch long.
Morphology: some nonspecific ST-T wave changes but nothing terrible
Final Read: Normal Sinus Rhythm with a left axis and right on the boarder for a 1st degree AV block
“ATTENTION: CODE BLUE CT 2 CODE BLUE CT 2” The hospital voice calls out
“Doc, that’s your seizure patient!” the nurse calls to the intern and senior resident as she runs over to the CT scanner. You follow over with the rest of the team.
“What’s going on?” You hear the senior ask a slightly chaotic sight. The patient is sitting in his stretcher and talking to the CT tech, who looks very anxious.
“It was the strangest thing doc. I was talking to him, and then all of a sudden, he just stopped responding and slumped over. His extremities started shaking and he looked a little gray. I looked at his monitor and it looked like he flat lined! I ran to call a code blue and by the time I got back to him, he was totally back to normal. I’ve never seen anything like it. I was only gone a few seconds to call for help or I would have started CPR!” The tech tells you.
“Let’s get this patient back to his room NOW, get a crash cart, put the pads on him and then we’ll pull up the telemetry strips.” You hear your senior resident direct the room.
“No problem!” the patient’s nurse responds as she pushes his stretcher back to the main ER as you see the intern and senior resident pull up the tele strips.
“Here’s the rhythm strip off of the patient’s ECG, what do you notice?” the senior resident asks:

“Well… It looks like sinus rhythm with maybe a 1st degree AV block and a rate around 80?” he responds.
“Ok, good, now take at the tele strips from when the patient went to CT. I marked when he went unresponsive with the blue arrow” she tells the intern.


(Please note, this is one long strip, but due to size, I had to cut it in half)
“Wow that looks much different. His heart rate drops to the 30s and then the pauses are very, very long. No wonder he went unresponsive. He wasn’t perfusing his brain at all!”
“Exactly! So, was he having seizures?” She asks?
“Uh… No? I guess not. Oooooohhhh. This was convulsive syncope! That’s why he didn’t really have a post-ictal period. Now I get it. That makes way more sense than a new onset seizure disorder in his 90s.” The intern responds.
“I mean, it’s not impossible to have your first seizure in your 90s. Remember, we still have to consider things like a mass, bleed, toxins, infection, and more, but based on these tele strips and what the CT tech saw, I think we have the right answer. Now go give EP a call so we can get a pacing wire in this poor guy before he flatlines again…”
Before we wrap up, let’s define what’s going on. The above case is an example of sick sinus syndrome. Classically, with sick sinus syndrome, we expect progressively worsening sinus bradycardia. It can lead to sinus arrest and potentially syncope, as we see above. Notice how our patient’s tele strip progressively slows down until the beats are very far apart.
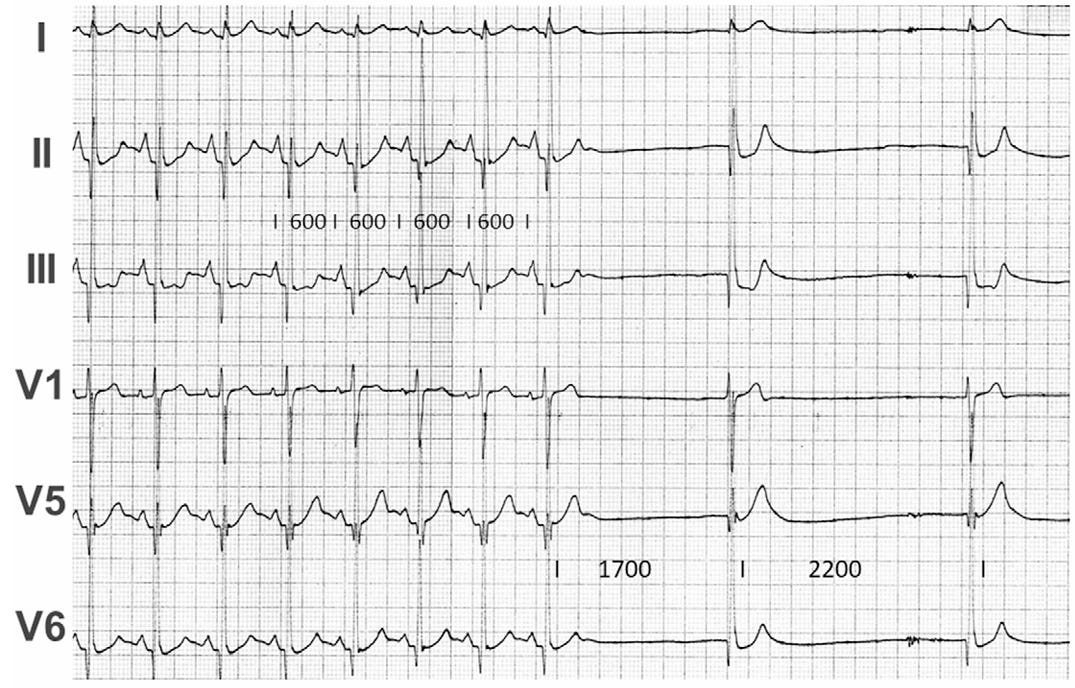
Sometimes you don’t get to see a progressive slowing of the beats before a pause. In 2020, The Journal of Electrocardiology presented 2 cases of syncope due to sudden, unexpected sinus arrest. Interestingly, Dr. Wellens (of the Wellens’ Waves) is the senior author of the paper.
His paper shows two cases where the heart just decided to take an unexpected break. Here’s one of the ECGs from his paper:
Ref: https://www.sciencedirect.com/science/article/abs/pii/S0022073619308313?via%3Dihub
Notice in the strips here, the patient is in sinus rhythm and then there are pauses with escape beats. This pause with escape beats, which lasted 12 seconds, caused a syncopal event. This patient in now the proud owner of a shiny new pacemaker!
Case Wrap up:
“Hello, uh.. Cardiology? This is one of the interns in the emergency department. I have a patient to discuss with you in bed 12. He’s a 95-year-old male coming in with convulsive syncope. I think he’s developed sick sinus syndrome and is having long pauses on the monitor. When he gets these pauses, he passes out and shakes a little bit. Family initially thought it was seizures but we saw one of these episodes, caught it on tele, and found the culprit. We have him on the monitor with pads in place, ready to pace if needed. You’ll come down and assess? Thank you!
Recap:
1) Not everything that shakes is a seizure. Consider convulsive syncope in your differential
2) Sick sinus syndrome is usually marked by progressive slowing of the heartrate however, sometimes, the heart just stops unexpectedly!
3) If you have a patient having unexplained events, don’t forget to keep him or her on telemetry when he or she goes to CT!
4) As we come to the end of the academic year, congratulations to those who are graduating! Don’t forget to update your email address to keep getting these cases!
Hit me up with any questions,
Lloyd
_________________________
Lloyd Tannenbaum, MD
This case nearly went the wrong way because the answer was never in the patient at rest. A normal exam, a normal resting ECG, a man sitting comfortably in his room: every static measurement was reassuring, because the etiology only existed for ninety seconds at a time. A seizure workup hunts for something that persists, a mass, a bleed, a metabolic derangement. This diagnosis lived only inside the episode.
The skepticism mattered, the senior was right to balk at a first seizure at 95, but suspicion alone could not close it. The finding still lived inside an event no one could produce on command. What broke it open was keeping the patient monitored long enough that the next episode happened while the strip was running. The CT tech saw the truth before anyone deduced it.
That is the quiet weight of recap point three. When the decisive finding is transient, you cannot reason your way to it from a calm exam. You have to stay instrumented until the event repeats and shows you what it is.