
It’s How Long?!
I’m not impressed, I’m worried!

“It’s happening again, go get the resident! NOW!”
You look up from your desk and hear commotion coming from the resuscitation bay. All of a sudden you see a nurse sprint over to one of the interns, urgently say something, gesture back at the bay, and rush off.
“Find the chief resident NOW and tell her to meet me in room 3 STAT” you hear the intern tell the medical student and run off.
The medical student scurries off and suddenly you see the chief and student running to bay 3. Intrigued, you go follow and nod to Scott, the pharmacist, who follows you.
As you walk in, you hear, “He’s back in Torsades. Wait. Now he’s out of it again. It only lasts about 30 seconds. I told you to give him magnesium. Did you give him mag?” the chief barks at the intern.
“I did!” The intern said.
“Did you give him more mag after that?” the chief asks.
“He’s been given 6 grams of magnesium in the past 2 hours at this point! Isn’t that enough magnesium? Is there anything else we can do?” you hear the intern ask.
“What’s going on, guys?” you ask, as you step towards the patient.
“I’ll manage the patient; you catch the attending up” the chief instructs the intern.
“Sure!” The intern responds. “This is Jason, he’s a 56 year old male who was working at a construction site. According to his co-workers, he’s a model employee. Never late, always polite. Today, he was acting strange. Seemed a little out of it, not quite himself, according to his boss. He was driving a bulldozer when suddenly there was a loud crash. He drove right into the wall of the structure they were building. He came in unresponsive as a major trauma alert. He was intubated emergently here. Imaging was negative, no signs of any injury. But he keeps going into Torsades. We can’t figure out why and we can’t seem to keep him out of it.”
“What did his ECG look like when he got here?” You ask the intern.
“Here it is, take a look:”
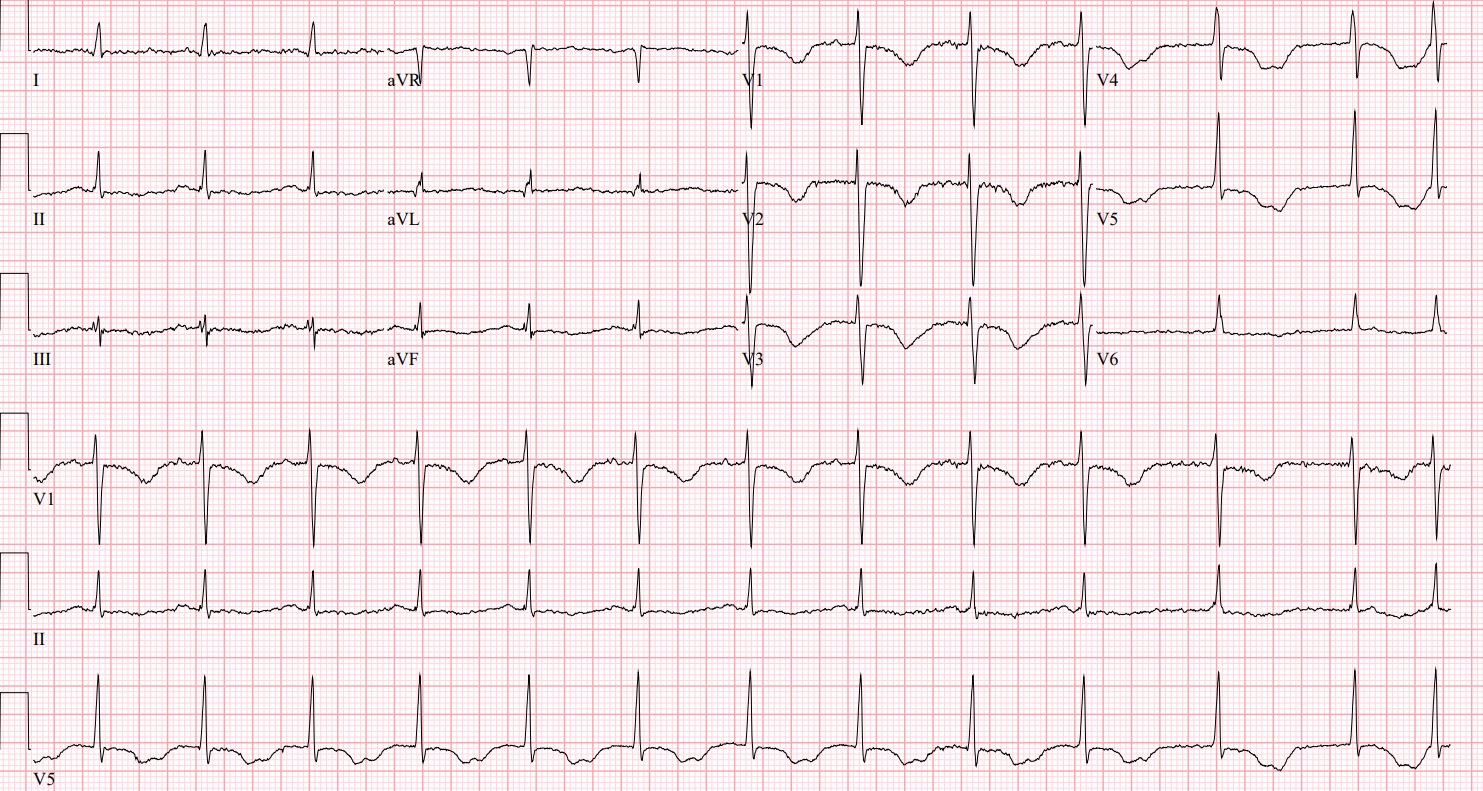
Rate: 77-80 beats per minute
Rhythm: Sinus rhythm
Axis: Normal axis
Intervals: PR looks ok, QRS is narrow. QTc is long!
Morphology: Some nonspecific ST-T wave changes. The T wave is inverted in the anterior leads
Final read: This patient is in sinus rhythm with a prolonged QTc. The computer is reading: QT/QTcB: 544/612 which is super long!
(Side note, what is QTcB? That means that the computer is using Bazett’s Formula to compute the QTc. MDCalc walks you through computing a QTc here using several different formulas. This formula is the traditional formula, often used by most automated ECG machines.)
“Why is his QT Interval so long?” You ask the intern. “Does he have a history of this?”
“Yes!” The intern replies. “He has known congenital long QT Syndrome. He’s well known to cardiology. Never had any trouble with it. He was on beta blockers for years to prevent arrhythmias which worked really well. According to his girlfriend, he’s having some money issues and couldn’t afford his medications anymore. He’s been off his meds for about 2-3 weeks now… and this is what happened.”
“He’s going back into Torsades again! Story time is over, get over here and help me!” You hear the chief resident call out.
Taking a look at the telemetry strip, you see:
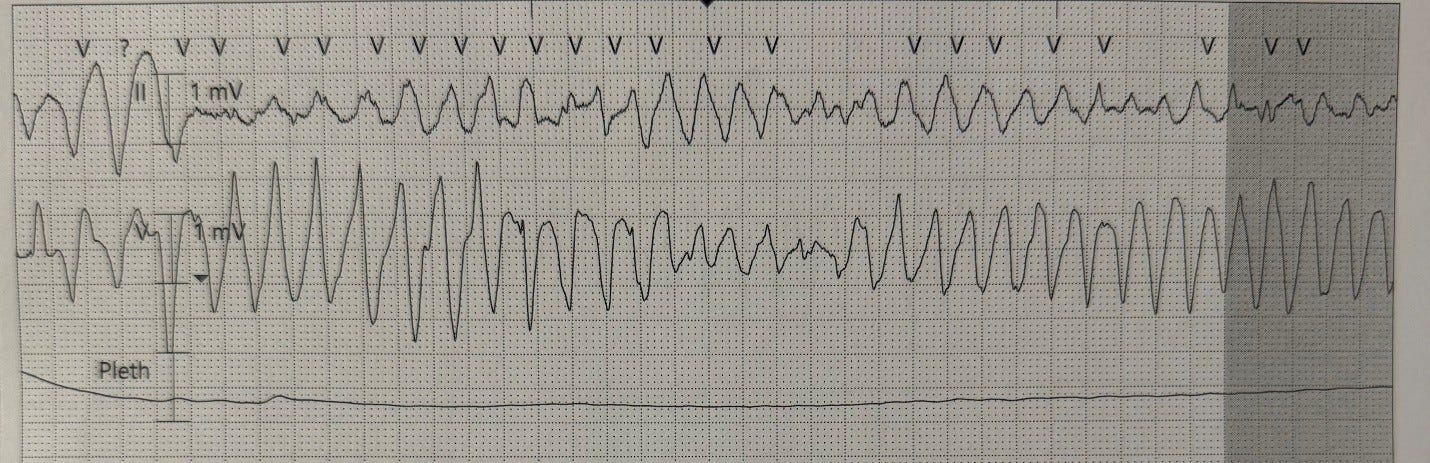
“Yup, he’s definitely in Torsades!” You say, “What have we done already for him?”
“He’s gotten a total of 6 grams of magnesium. His potassium is 4.0. We’ve gotten him as optimized as we can. What else can we give him?” the intern wonders.
“What about isoproterenol?” the chief resident asks. “We used it in the ICU once for refractory Torsades, do you think that has a role here?”
You notice Scott start to twitch.
“Great question!” you reply. “Scott, do you want to play too or just listen to me make up pharmacological advice and wince quietly?”
“I like to let your residents finish their sentences before cutting them off; it’s called gentle teaching and basic manners. Anyway, it sounds like you and the intern already have the basics covered in terms of aggressively managing the magnesium, potassium, and calcium as we know any deficits in these can significantly worsen the situation. I’d recommend checking a magnesium level and utilizing 3.5 – 5 mg/dL as a therapeutic target range with considerations for a magnesium infusion to maintain that if the renal function is good (GFR >30 ml/hr).
We also want to consider if there are any other precipitating factors such as hypothermia or, as we often chat about, QTc prolonging medications. Once I’m done taking up a significant part of your day over-explaining, I’m going to review the medication records to see if there are any antiarrhythmics, antifungals, fluroquinolones, macrolides, high-risk psych medications, antihistamines, methadone or any other miscellaneous medications that might show up as high risk on a database like CredibleMeds for QT prolongation.
In some cases of Torsades, chronotropic therapy (drugs to increase the heart rate) may be beneficial; however, as the intern pointed out, this patient has a history of congenital long QT so this is not going to be a good idea here. As your chief mentioned, isoproterenol is a very potent chronotropic medication, in fact, it’s a beta agonist, the complete opposite of a beta blocker.
Isoproterenol a good idea, but, it is often avoided in congenital long QT as in this subset of patients it can induce Torsades! Oops. It is, however, frequently used in refractory Torsades due to an induced prolonged QT interval.
(BONUS SCIENCE: there are several different types of congenital long QT syndrome, the most common of which are LQTS1, LQTS2, and LQTS3. In LQTS1 and LQTS2, adrenergic stimulation (such as isoproterenol) can induce Torsades, but in LQTS3, pauses and slow heart rates tend to induce Torsades, so isoproterenol may actually be beneficial. This distinction is beyond the scope of this write up, but for more, see this paper.)
Having said all that, I do have ONE infusion in my bag of tricks that may help us out: Lidocaine! While the other anti-arrythmias like amiodarone would send our QT in the wrong direction, lidocaine is the preferred anti-arrhythmic for patients with a congenital long-QT syndrome. This can be given at the typical one milligram per hour infusion and the patient already received the 1 – 1.5 mg/kg loading during ACLS protocol.
Remember, if medications don’t work, you guys can consider overdrive pacing to prevent further runs of Torsades. If we increase the heart rate, we shorten the QT interval, which should decrease the occurrence of the R on T phenomenon,” Scott finishes up.
Case Wrap Up
“Wow, Scott, that was a lot of words to say, ‘Hey guys, probably shouldn’t do isoproterenol on this patient, Lidocaine would work better,” you say.
“Just shut up and float a pacer. You’re already holding the kit, we all know you’re going to use it. I’ll prep the lidocaine drip.” Scott fires back
“What happened to gentle teaching?” you ask.
You can’t make out exactly what Scott said as he walks off to get the medications ready, but it likely wouldn’t have been printable anyway.
Recap:
Initial steps for patients having runs of Torsades De Points is to make sure all electrolytes are optimized
Magnesium is the initial therapy of choice
In refractory Torsades, it is very important to know what is causing the dysrhythmia
In acquired prolonged QTc, isoproterenol (a beta agonist) is a reasonable choice to speed up the heart rate and shorten the QT interval
In congenital prolonged QTc, be careful with isoproterenol, as it can induce Torsades in certain patients
Lidocaine is the preferred antiarrhythmic for patients with refractory Torsades and congenital long QT
Overdrive pacing is a reasonable consideration for patients in refractory Torsades, as it increases the heart rate and shortens the QT interval
Selected references from Snarky Scott:
Thomas SH, Behr ER. Pharmacological treatment of acquired QT prolongation and torsades de pointes. Br J Clin Pharmacol. 2016 Mar;81(3):420-7. doi: 10.1111/bcp.12726. Epub 2015 Oct 26. PMID: 26183037; PMCID: PMC4767204.
Wilde AAM, Amin AS, Postema PG. Diagnosis, management and therapeutic strategies for congenital long QT syndrome. Heart. 2022 Mar;108(5):332-338. doi: 10.1136/heartjnl-2020-318259. Epub 2021 May 26. PMID: 34039680; PMCID: PMC8862104.
Farkas J. Torsade de pointes. EMCrit Project.
Hit me up with any questions,
Lloyd
Heading to ICEM 2026 in Hamburg, Germany this year? I’ll be speaking at the Emergency Cardiology Challenges Workshop on 9 June 2026 with Dr. Amal Mattu and friends! Come say hi!
**Looking for a dynamic guest lecture on Emergency Cardiology for your Grand Rounds? Reach out here for a lecture request by Dr. Tannenbaum. If you have reached out already, I have emailed you back. If you haven’t gotten it, please message me directly on Substack or just reply to this email.**
Good call with the lidocaine. Mexilitine may work even better. The long diastole that accompanies LQT actually enhances the block provided by the Class 1B antiarrhythmic. The perfect antiarrhythmic (if there is such a thing) includes an inactivated state Na channel blocker to block the Na/Ca exchanger from going into reverse mode and adding to the afterdepolarizaions that can accompany LQT.