


VTach or something else?

This EKG is a repeat from the last post. As promised. We're going to take a deeper dive into VTach. Take a look:

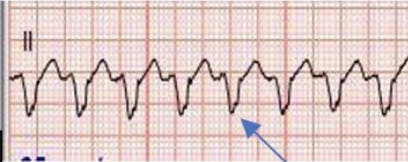
Here's my read:
Rate: 180 ish
Rhythm: NOT sinus
Axis: Probably left axis, but likely not clinically significant
Interval: Widened QRS complexes, no obvious P waves, no PR interval
Morphology: Most beats looks the same but the 10th and 13th look different
Final read: This is a wide complex, regular tachycardia but is it consistent with VTach? Or SVT with aberrancy? Or something else?
Before we dive into the amazingness that is VT (yes it's my favorite arrhythmia), what is SVT with aberrancy? Well, aberrancy just means that there is some kind of aberrant (or non-traditional) conduction. Think SVT with a bundle branch block. So is this EKG more likely VTach? Or SVT with a left bundle branch block? To be determined...
Let's jump in. First of all, from the ER's point of view, if the patient is unstable, we always assume that a wide complex, regular (also called monomorphic) tachycardia is VTach until proven otherwise (often by Cards in the EP lab). But let's take a look into EKG findings that can point us towards VTach in those rare moments where we have time to scrutinize the EKG.
Take a look at the following rhythm strip:

I promise this one is VTach. It may not look like it and the QRS complexes may look confusingly narrow, but that's because it's from a 2 day old who just came out of surgery to fix transposition of his great vessels. In a kiddo this size, anything over 80msec is wide. And, as the former resident on the PICU who spent a very very long time working with the zoom function and calipers, I promise, the QRS is more than 80 msec and is therefor wide.
Notice the "F" and the "C" beats and how they look different from the rest of the beats. The "F" stands for fusion beat and the "C" stands for capture beat
Fusion beats: occur when a ventricular beat and the sinus node fire at the same time and the resulting complexes "Fuse" together giving you a beat that looks like a mix of a ventricular beat and a sinus beat. It's one of those weird things in medicine that are actually appropriately named.
Capture beats: occur when the SA node "captures" the heart's conduction system and it looks like a traditional sinus beat in the middle of a run of VTach
If you see either of these in the middle of a run of a wide complex, regular tachycardia, it's a slam dunk for VTach, every time.
What else can tip us off for Vtach? Take a look at this strip. It's coming from a 19 yo M coming in with syncope:

Well, there's a positive blue arrow sign, so that must mean something. This guy was having runs of Vtach leading to syncope. When we got this EKG, we found A-V dissociation (the p waves are pointed out with blue arrows and don't relate to the QRS complexes at all). If you see A-V dissociation, it's another tip off for VTach.
There are two other signs to be aware of if you're looking to distinguish between VTach and SVT with aberrancy that can aid you. I don't find them very exciting though:
and

What are we seeing? Squiggles with arrows and lines of course.
The first picture on the Left is called "Josephson's sign" which just means that there is notching at the nadir (lowest point) of the S wave.
The picture on the Right is called "Brugada's Sign" which says that the time from the onset of the QRS complex to the nadir of the S wave is over 100 msec.
I know. really not exciting.
I know what you're thinking. Capture beats, fusion beats and A-V dissociation are way cooler. I know, I agree.
So now what?
Well, for completion's sake, here is a link to the Brugada Criteria for VT (Yes, those Brugada brothers of EKG fame): https://www.mdcalc.com/calc/4045/brugada-criteria-ventricular-tachycardia You can use it to help walk through an EKG that you're puzzling through to see if it's leaning more towards VT or SVT with aberrancy. If you're super curious, I attached the article by Drs. Brugada from 1991 describing their process for walking through a wide complex monomorphic tachycardia and how they developed their criteria. I think it's neat, but I like wiggly lines.
So what about the EKG at the top of this email? If you look closely at beats 10 and 13, they're fusion beats, which lead to a diagnosis of VTach! Big thanks to Dr. Dan Toren for sending this ekg!
Remember, determining between VTach and SVT with aberrancy is challenging and often more of an art than a science. Let's wrap it up and review:
***From the ER's point of view, if the patient is unstable, treat a wide complex monomorphic (regular) tachycardia like VTach every time***
When you have time to look closely, here are some signs that can help you clinch the diagnosis of Vtach:
Capture beats
Fusion beats
A-V Dissociation
Josephson's sign
Brugada's sign
***From the ER's point of view, if the patient is unstable, treat a wide complex monomorphic (regular) tachycardia like VTach every time***
Hit me up with any questions,
Lloyd
________________________________________________
Lloyd Tannenbaum, MD
Assistant Program Director
A new approach to the differential diagnosis of a regular tachycardia with a wide QRS complex