
Wait, where did that STEMI go

Shout out to my new friends at GWV for handling this case like a boss (and taking the time to send me the EKGs)! Take a look:
EMS calls and says they're heading to you real quick. They have a 60 yo F with chest pressure, shortness of breath, diaphoresis and she doesn't look good. They transmit you her EKG, take a look:
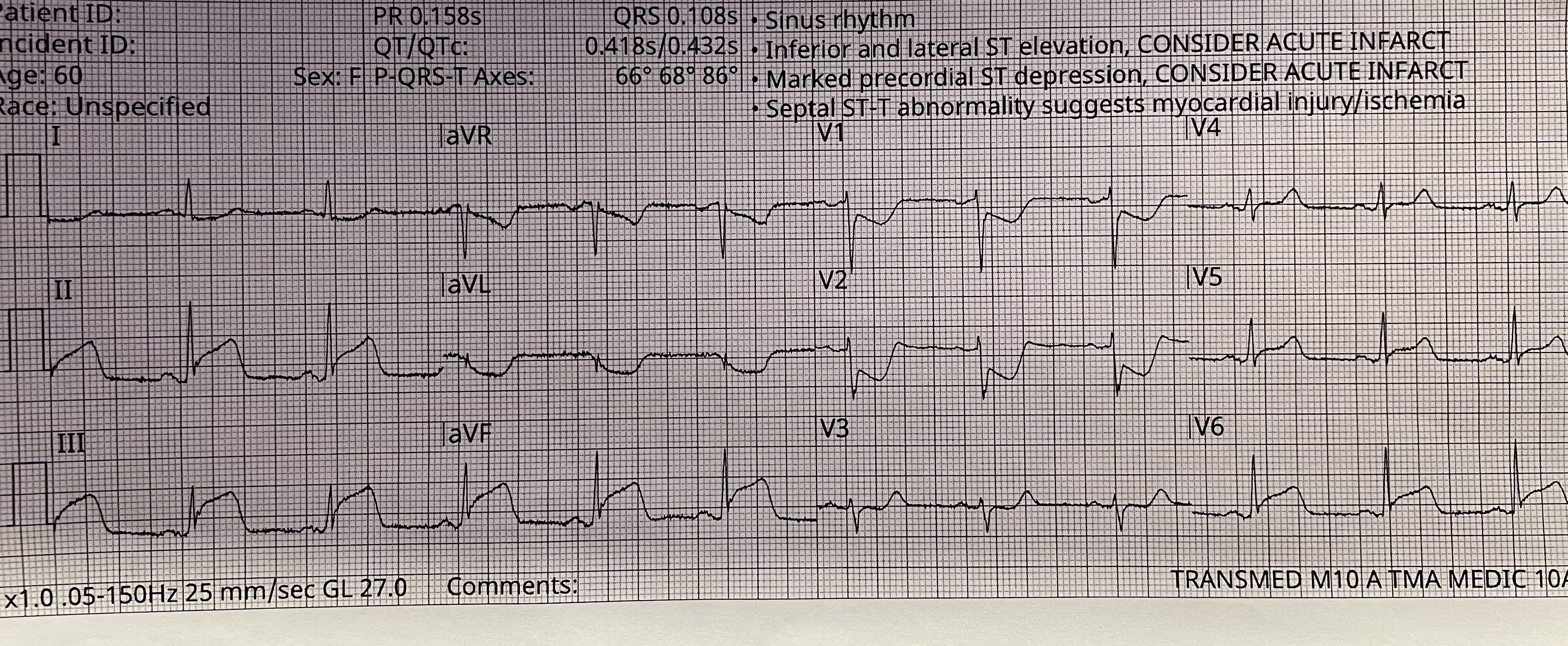
Looks bad right? Here's my read:
Rate: 70ish
Rhythm: NSR
Axis: normal
Intervals: Narrow QRS complexes, reasonable PR interval
Morphology: Impressive ST Segment elevation in II, III, aVF with ST depression in V1 and V2
Final read: This EKG is consistent with an Inferior STEMI. You could convince me easily that there is posterior involvement given the ST depressions in V1 and V2 also
EMS asks you to active the STEMI team and be ready for them, they're hustling.
EMS arrives approximately 12 minutes after that first EKG. Your team is ready, they hook the patient up to the monitor, repeat the EKG and this is what you see:
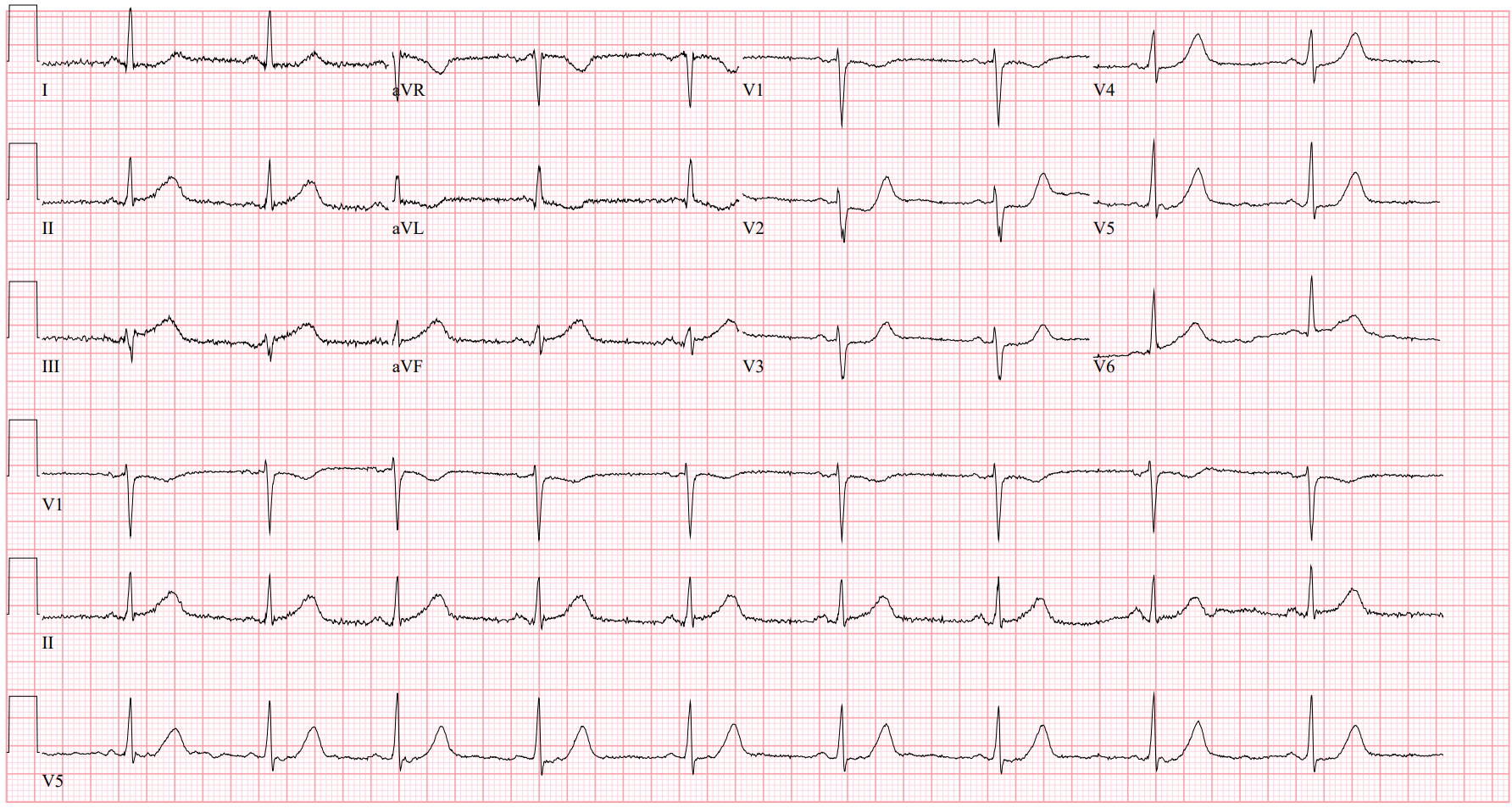
Well.. That's awkward. what's going on now?
Rate: 55
Rhythm: NSR
Axis: normal
Intervals: Narrow QRS, nl PR
Morphology: The impressive ST segment changes that were in the previous EKG have now mostly disappeared. There is still a little ST elevation in III and a little bit of depression in V2 and maybe V3/V4
Final read: Sinus brady with nonspecific ST-T wave changes. This EKG ALONE doesn't meet criteria to activate the cath lab
Well shoot. Now what? The whole cath team is here. Do we send them home? "Hey STEMI team, sorry, we fixed her without you! bye!" Or should we still send her to Cath? That first EKG is scary. Right?
Well, for better or for worse, this phenomenon, coined by some as a "Transient STEMI" is not uncommon. There's a paper from 2008 that estimates approximately 6% of all STEMIs are transient STEMIs and up to 24% of high risk NSTEMIs are truly transient STEMIS in disguise. But what do we do with these patients?
Well, this is a hot topic amongst interventional cardiologists. There was a trial published in 2019 called the TRANSIENT trial, and for the first time ever in medical history, the name is actually indicative of what the authors studied. This study looked at 142 patients with a transient STEMI. Half were taken immediately to the cath lab for angiography and intervention while the other half were scheduled for a delayed cath. This study found no difference in major adverse cardiac events (MACE), defined as death, reinfarction, or target vessel revascularization at 30 days in either treatment group. A follow up study was performed looking at these patients one year later and still found no statistically significant differences in MACE between the delayed and immediate groups (5.7% vs 4.4% respectively)
So we can wait for cath, right?
Well, we don't know. The was a good ECG of the Month from Annals (attached) that walks through all of the different studies that have looked at transient STEMIs and what to do with them. There is just as much data pushing To cath emergently as there is To cath urgently. So what is the right answer? For now, I'd argue that it's a healthy conversation with the interventionalist on call and make a team decision that's best for the patient. From what I can find and from what I've been anecdotally told, when the ST Elevation recurs and when the patients have ongoing ischemic symptoms (think chest pain, diaphoresis, shortness of breath, etc), cards leans more towards emergent cath, but, again, there are no definitive guidelines in place as of yet.
Interestingly, the patient had one more EKG taken before the team decided to take her to cath, take a look:
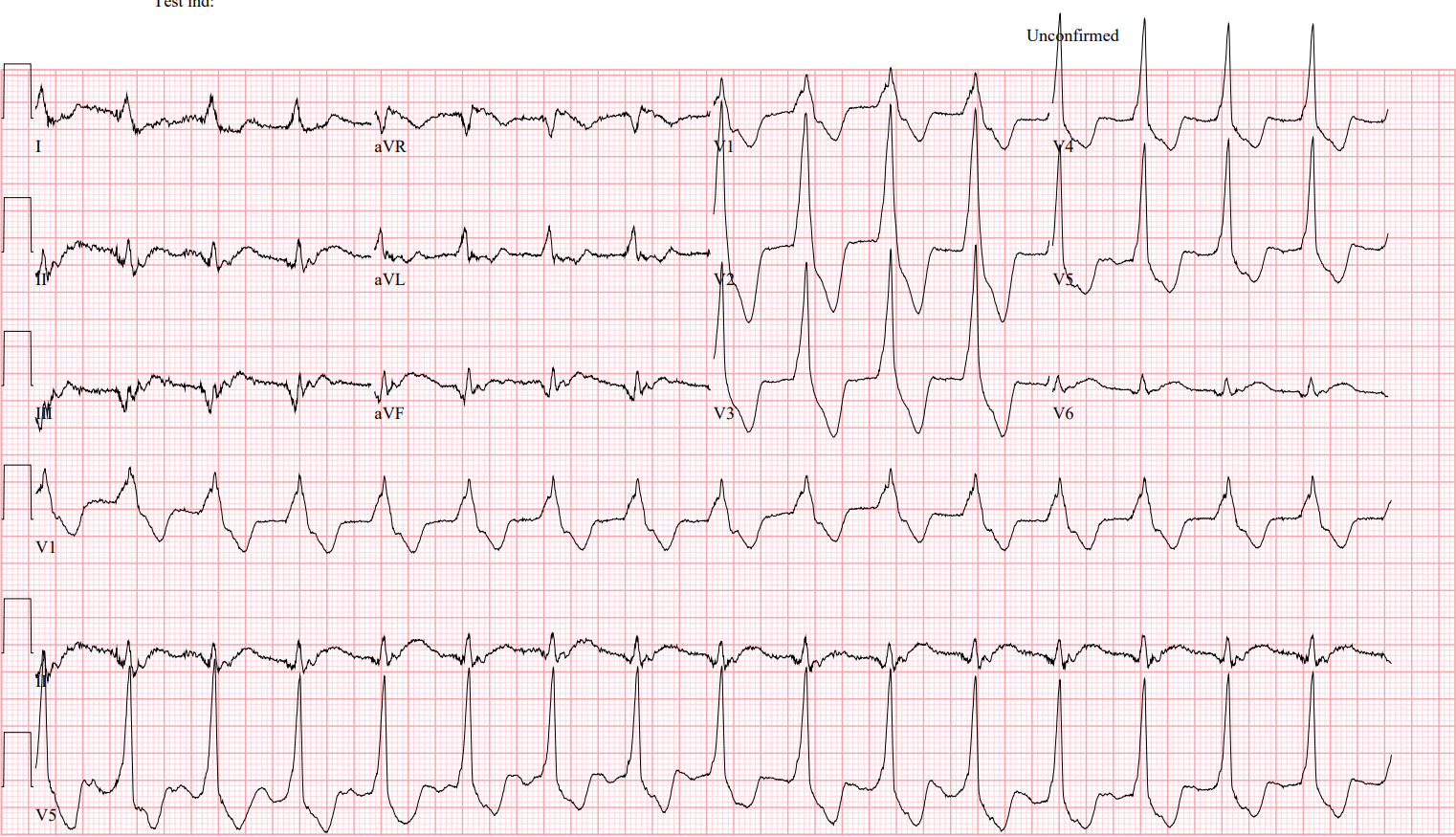
What's going on here?
Rate: 95 ish
Rhythm: No P waves, some kind of junctional?
Axis: normal? Maybe. Likely not super helpful
Intervals: WIDE QRS complexes
Morphology: It looks like VTach. But it's too slow...
Some of the doctors who trained before cath labs will probably recognize this rhythm. This is AIVR or Accelerated IdioVentricular Rhythm. Cool cool, but what do we do with it?
Nothing! It's traditionally a self-limiting arrhythmia known as the reperfusion arrhythmia. Classically seen after giving lytics in patients with an MI. If you see it, leave it alone! Antiarrhythmics, such as amiodarone, tend to cause hemodynamic collapse, which is .. bad.
So what happened to the patient? She was taken emergently to cath and found to have a 100% thrombotic occlusion of the Left Circumflex, which was stented successfully. Terrifyingly, she also briefly went into a VFib arrest, which highlights again that these patients can be tricky and need a good conversation with the interventionalist to determine if their preference is taking the patient to cath emergently or medical management until performing an urgent cath.
Hit me up with any questions,
Lloyd
_________________________________
Lloyd Tannenbaum, MD
APD, Emergency Medicine