


Sgarbossing it up!

“Scott, you’re so dramatic. 100 micrograms and 100 mg are practically the same…
“THIS IS PARAMEDIC 1015 REQUESTING EMERGENT MEDICAL COMMAND. Over.”
Well damn. Guess this argument with Scott over drug dosing is going to have to wait. You hustle over to the EMS phone and see your charge nurse, Shannon, walk over to listen in. “Go ahead medic 1015!”
“Hey Doc, we got a real sick one here and need some help. Mrs. Sloan is a 70-year-old female who called us for chest pain and shortness of breath. She has crushing chest pain and is barely able to speak, she’s so out of breath. This all started acutely tonight. She was at a dinner party, started dancing and then had sudden onset, severe pain and could not stop sweating. We arrived on scene about 5 minutes ago. Her blood pressure is 60/palp, she’s in and out of consciousness, pale, and diaphoretic. We sent you her ECG, it doesn’t look good. What do you want us to do?”
“Standby for one second Medic 1015, let me look at this ECG.”

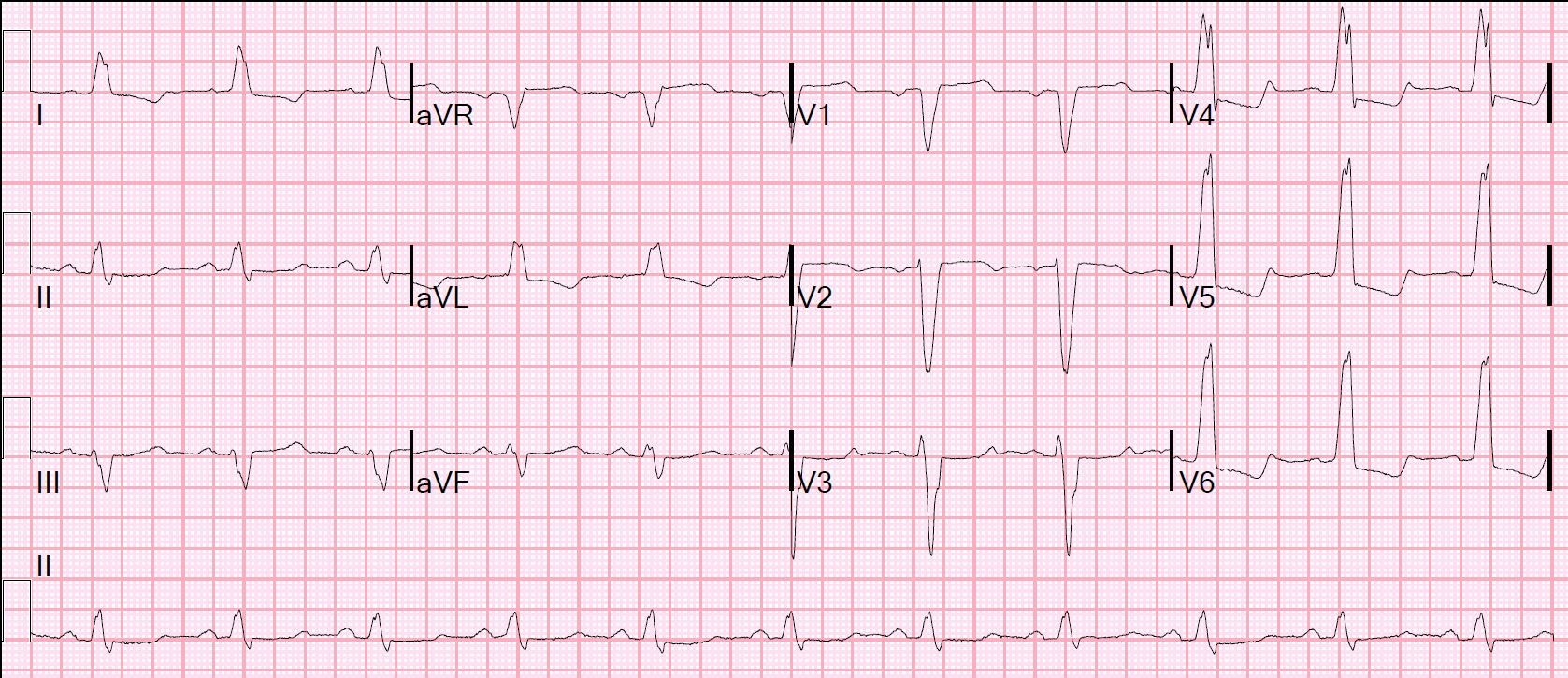
Rate: 100 ish
Rhythm: Sinus rhythm bordering on sinus tach (P before each QRS complex, 1-1 ratio P-QRS waves and upright P in lead II)
Axis: Left (QRS mostly up in I and down in aVF)
Intervals: WIDE QRS (QRS duration is 150msec)
Morphology: It looks like a left bundle branch block (LBBB) but the ST segments don’t look quite right
Final Read: Normal sinus rhythm with a LBBB and abnormal ST segments
Take a second and refresh yourself on EKG changes in an LBBB. Let’s take a look at a normal left bundle branch block together:
Rate: 72
Rhythm: Normal sinus
Axis: Left axis
Intervals: Widened QRS axis, normal PR, QTc looks ok
Morphology: A left bundle branch block is present. Notice how the QRS complex have a very high voltage and the ST segments are appropriately elevated or depressed in the opposite direction of the QRS complexes (more on this below).
Final read: This is normal sinus rhythm with a left bundle branch block.
Remember, in a LBBB, the Left Bundle is blocked (what a clever name), so the electricity flows SA node to AV node, there's a slight pause (The AV delay) and then down the bundle of His and then the right bundle. The left bundle is blocked, so the heart uses muscle-to-muscle spread to conduct impulses from right to left, which makes very large, wide QRS complexes.
But what is going with the ST segment elevations (V1, V2) and depressions (I, V4, V5, V6) in the normal LBBB above? This EKG is following the law of appropriate discordance. Remember, for a LBBB, there is a TON of electricity required to activate the entire myocardium of the left ventricle using muscle to muscle spread. This is shown on the EKG as very high voltages and a widened QRS. All of this electricity will naturally elevate the ST segment AWAY from the direction of the QRS complex in the anterior leads and will depress the ST segment AWAY from the direction of the QRS complexes in the lateral leads. Let’s turn all that text into a picture:
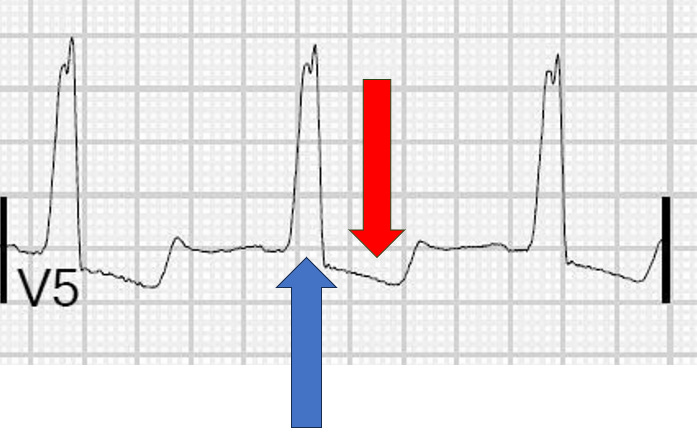
The BLUE arrow highlights that the QRS complex is positive (or, more scientifically, the majority of the QRS complex is positively deflected away from the baseline), where as the RED arrow highlights that the ST Segment is depressed away from the baseline. This is good, the QRS complex should go one way and the ST segment should be elevated or depressed AWAY from the QRS complex. V5 follows the Law of Appropriate Discordance.
But if there’s natural ST segment elevation and depressions all over a left bundle branch block, how do we know when a patient is having a STEMI or not?
Enter the Sgarbossa Criteria. First defined by Dr. Elena Sgarbossa in 1996, these criteria were designed to help clinicians navigate the complex world of acute myocardial infarctions in the setting of a left bundle branch block.
The original criteria are:
Concordant ST Elevation >1mm in a lead with a positive QRS Complexes
Concordant ST Depression >1mm in leads V1-V3
Excessively discordant ST elevation >5mm in leads with a negative vector QRS Complex
***REMEMBER: to be Sgarbossa Positive, you just need to hit criteria in just ONE LEAD, not two contiguous!***
So let's look through the ECG medic 1015 sent us. Notice in leads V2 and V3, the ST segment is depressed TOWARDS the QRS complex. I’m going to highlight lead V3:

The BLUE arrow highlights that the QRS complex is negative; the RED arrow highlights that the ST Segment is depressed TOWARDS the QRS complex. This is BAD. This is called CONCORDANT ST segment depression. This ECG is Sgarbossa positive; Activate the cath lab!
But what about the third criterion? The original Sgarbossa Criteria defined excessively discordant ST Elevation as >5mm in leads with a negative QRS complex. Here’s an example of an ECG that would meet that third criterion:

Looking at this picture, the BLUE line shows the ST segment, the GREEN line shows the T-P segment (the baseline). The red line shows the degree of ST segment elevation and notice that it is larger than one large box (or 5 small boxes) which is greater than 5 mm.
Unfortunately, this last rule of the original Sgarbossa criteria didn’t perform as well as the first two and Dr. Stephen Smith, of Dr. Smith's ECG blog, modified that rule, and his modification has replaced the original rule. The modified rule is:
≥ 1 lead anywhere with ≥ 1 mm STE and proportionally excessive discordant STE, as defined by ≥ 25% of the depth of the preceding S-wave.
Here's a picture from Dr. Smith's paper of how to calculate this modification (both image A and B would be positive by this modification):
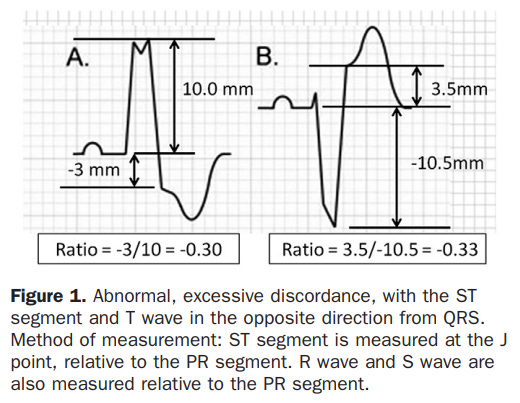
Image cite: Smith SW, Dodd KW, Henry TD, Dvorak DM, Pearce LA. Diagnosis of ST-elevation myocardial infarction in the presence of left bundle branch block with the ST-elevation to S-wave ratio in a modified Sgarbossa rule. Ann Emerg Med. 2012 Dec;60(6):766-76. doi: 10.1016/j.annemergmed.2012.07.119. Epub 2012 Aug 31. Erratum in: Ann Emerg Med. 2013 Oct;62(4):302. PMID: 22939607.
***REMEMBER (I'm going to say it again, this is important): to be Sgarbossa Positive, you just need to hit criteria in just ONE LEAD, not two contiguous!***
“HEY DOC!” you hear Shannon yell, “Are you still with us?? We need some medical command please! Stop staring at ECGs and say something.”
“Shoot, sorry medic 1015! Looking at the ECG you sent us, this patient is Sgarbossa positive and we need to let the heart team know. I’ll activate the cath lab. How are your vitals?”
“Doc, based on what you’re saying, she’s probably in cardiogenic shock. BP is 70/30, heart rate is about 100, she’s still in and out of consciousness. We’ll be to your door in about 5 minutes.”
“That’s not good. Hang 500 cc of IV fluid and spike a bag of Norepi. Try to use the norepi to get her blood pressure higher. Put her on a non-rebreather and assist her ventilations with a BVM if necessary. I’ll have the resus bay ready and we’ll intubate before cath, if needed. See you in 5...
Sgarbossa Quick Review:
There are some natural ST segment elevation and depression expected with a left bundle branch block
Know the law of appropriate discordance and look at every LBBB that comes across your desk to get a good idea of what normal is
You run into trouble with a LBBB when it breaks the law of appropriate discordance
Remember the first 2 Sgarbossa Criteria
Concordant ST Elevation >1mm in a lead with a positive QRS Complexes
Concordant ST Depression >1mm in leads V1-V3
The third Sgarbossa Criterion was modified
≥ 1 lead anywhere with ≥ 1 mm STE and proportionally excessive discordant STE, as defined by ≥ 25% of the depth of the preceding S-wave.
The Sgarbossa Criteria are tricky. Don’t be afraid to look it up on shift if you have a questionable ECG or a patient with a concerning story
These ECGs aren’t very common! A huge thank you to the paramedics who took this ECG, recognized that it wasn’t normal, and called for backup!
Congratulations to everyone graduating from residency this week!
If you used your institutional email address, make sure to update it to keep getting EKG emails!
Hit me up with any questions,
Lloyd
**Looking for a dynamic guest lecture on Emergency Cardiology for your Grand Rounds? Reach out here for a lecture request by Dr. Tannenbaum**
_________________________
Lloyd Tannenbaum, MD
APD, EM Residency
Geisinger Wyoming Valley
Posterior mi was excluded with posterior leads for the first ekg?